by Alan S. Cajes

Note: The MMR in the Philippines was 209 in the early 90s. The target MMR for 2015 is at 52. “In 1998 MMR fell from 209 to 172 but seems to have plateaued thereafter stagnating at 162 in 2006. At this pace of reduction, by 2015 MMR will have only declined to 140 and the target of 52 will be unachievable.” About 4,600 women die giving birth each year in the country (http://philippines.unfpa.org/read_more.php?id=14). Picture shown is from UNFPA.
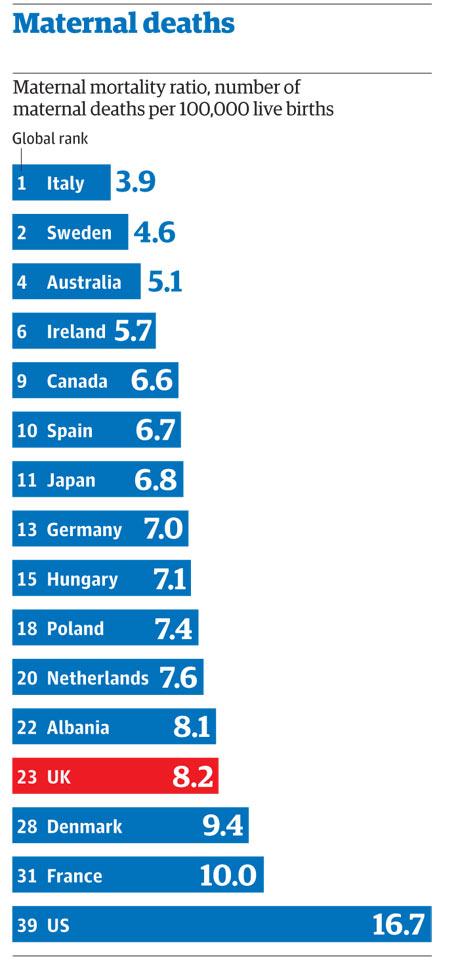
However, the UK-based Guardian published a study by Lancet on Maternal Mortality Rate (MMR) or the number of maternal deaths per 100,000 live births. According to the study, the MMR in the Philippines in 2008 is 83.6. The MMR in 1990 was 174.4. The 2008 MMR of the Philippines is slightly better compared to Fiji (85.4), but slightly worse compared to Peru (81.3). The other countries that have lower MMR than the Philippines include North Korea with 64.2, Cuba with 40.0, El Salvador with 37.1, Japan with 6.8, and Italy, which has the best MMR, with 3.9.
The Lancet study is entitled “Maternal mortality for 181 countries, 1980—2008: a systematic analysis of progress towards Millennium Development Goal 5” published online on 12 April 2010 under volume 35, issue 9726, pages 1609-1623. A report summary, which is lifted from the Lancet website, is provided below.
Background
Maternal mortality remains a major challenge to health systems worldwide. Reliable information about the rates and trends in maternal mortality is essential for resource mobilisation, and for planning and assessment of progress towards Millennium Development Goal 5 (MDG 5), the target for which is a 75% reduction in the maternal mortality ratio (MMR) from 1990 to 2015. We assessed levels and trends in maternal mortality for 181 countries.
Methods
We constructed a database of 2651 observations of maternal mortality for 181 countries for 1980—2008, from vital registration data, censuses, surveys, and verbal autopsy studies. We used robust analytical methods to generate estimates of maternal deaths and the MMR for each year between 1980 and 2008. We explored the sensitivity of our data to model specification and show the out-of-sample predictive validity of our methods.
Findings
We estimated that there were 342 900 (uncertainty interval 302 100—394 300) maternal deaths worldwide in 2008, down from 526 300 (446 400—629 600) in 1980. The global MMR decreased from 422 (358—505) in 1980 to 320 (272—388) in 1990, and was 251 (221—289) per 100 000 livebirths in 2008. The yearly rate of decline of the global MMR since 1990 was 1·3% (1·0—1·5). During 1990—2008, rates of yearly decline in the MMR varied between countries, from 8·8% (8·7—14·1) in the Maldives to an increase of 5·5% (5·2—5·6) in Zimbabwe. More than 50% of all maternal deaths were in only six countries in 2008 (India, Nigeria, Pakistan, Afghanistan, Ethiopia, and the Democratic Republic of the Congo). In the absence of HIV, there would have been 281 500 (243 900—327 900) maternal deaths worldwide in 2008.
Interpretation
Substantial, albeit varied, progress has been made towards MDG 5. Although only 23 countries are on track to achieve a 75% decrease in MMR by 2015, countries such as Egypt, China, Ecuador, and Bolivia have been achieving accelerated progress.
Funding
Bill & Melinda Gates Foundation.
According to the United Nations Population Fund (UNFPA):
“In the Philippines, while 40% of maternal deaths are unclassified, it is clear that hypertension (27%), hemorrhage (18%) and unsafe abortion (11%) are the three major causes of maternal mortality. All of these problems are preventable and can be addressed through adequate medical care such as the presence of skilled birth attendants, emergency obstetric care (EmOC), when necessary, and access to family planning services.” (See http://philippines.unfpa.org/read_more.php?id=14)
According to the Department of Health per its National Objectives for Health:
“The MMR between 1987 and 1993 was estimated at 209 per 100,000 live births. This improved to 172 per 100,000 live births based on estimates between 1991and 1997. A recent study based on the maternal causes of deaths in the civil registry estimated the MMR at 138 per 100,000 live births in 2002 (Ericta 2003).”
“Among Filipino women, the lifetime risk of dying from maternal causes is one in 100. Maternal deaths made up less than one percent of the total deaths in the country, but they contribute 14 percent of all deaths in women aged 15-49 years (NSO 1998).”
According to the National Statistics Office (NSO):
“In 2006 there were 1,721 maternal deaths reported to have occurred all over the country. Said number represented a decrease of 0.6 percent from the 2005 figure of 1,732. Maternal mortality rate (MMR) for the year was 103.5 deaths per 100,000 live births.”
“CALABARZON, which ranked second in terms of live births among the regions, reported the most number of maternal deaths at 247. Next to CALABARZON were Central Visayas (198) and National Capital Region (186).”
“Meanwhile, Bicol Region recorded the highest MMR of 165.8 followed by Eastern Visayas (147.0) and Caraga (135.7).”
The NSO Explanatory Notes on MMR state:
“Statistics for this vital event are based on information obtained from the Death Certificates (Municipal Form No. 103) transmitted by the City/Municipal Civil Registrars to the National Statistics Office for processing and archiving. Included in this report are maternal deaths that occurred in 2006 and were registered from January 2006 to March 2007. No adjustments for underregistration were done in the presentation.”
“Maternal death refers to the end of life of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.”
Although there is an absence of an absolutely reliable data on the actual maternal mortality rate as of today, any number on maternal mortality is unacceptable. The target should be zero mortality. That is the ideal scenario.
In our real world, however, we are witnessing the deaths of mothers during or immediately after the end of pregnancy.
How should we address this problem?
My humble opinion is to come up with case studies and practices related to MMR representing different segments of the population. It is not desirable to have a totalizing solution that assumes the factors leading to the MMR problem are the same everywhere in the Philippines. Case studies at the level of the provinces, cities, municipalities and barangays, with due consideration of levels of urbanization, are important to understand better the factors that contribute to MMR. Only then can we think of a better way to solve the problem.
As an example, a barangay-level study in Paranaque showed that MMR can be addressed by prohibiting home-based deliveries, providing access to facility-based delivery, and providing social health insurance to pregnant women, among others.
It seems to me that reducing MMR by decreasing pregnancy is a simplistic way of dealing with a highly complex phenomenon.
As an example, a barangay-level study in Paranaque showed that MMR can be addressed by prohibiting home-based deliveries, providing access to facility-based delivery, and providing social health insurance to pregnant women, among others.
It seems to me that reducing MMR by decreasing pregnancy is a simplistic way of dealing with a highly complex phenomenon.
See http://static.guim.co.uk/sys-images/Guardian/Pix/maps_and_graphs/2010/4/13/1271150525875/chilbirth-deaths-graphic-001.jpg; http://www.census.gov.ph/data/sectordata/sr11563tx.html
{kind=link}
No comments:
Post a Comment